Analysis by Keith Rankin.
These charts look at Covid19 incidence in China (the most important first-wave country, with a limited second wave), Italy (the lead second-wave country), and USA and Australia (second-wave countries – drawing their caseload from Europe – with limited first-wave exposure from Asia in January and February).
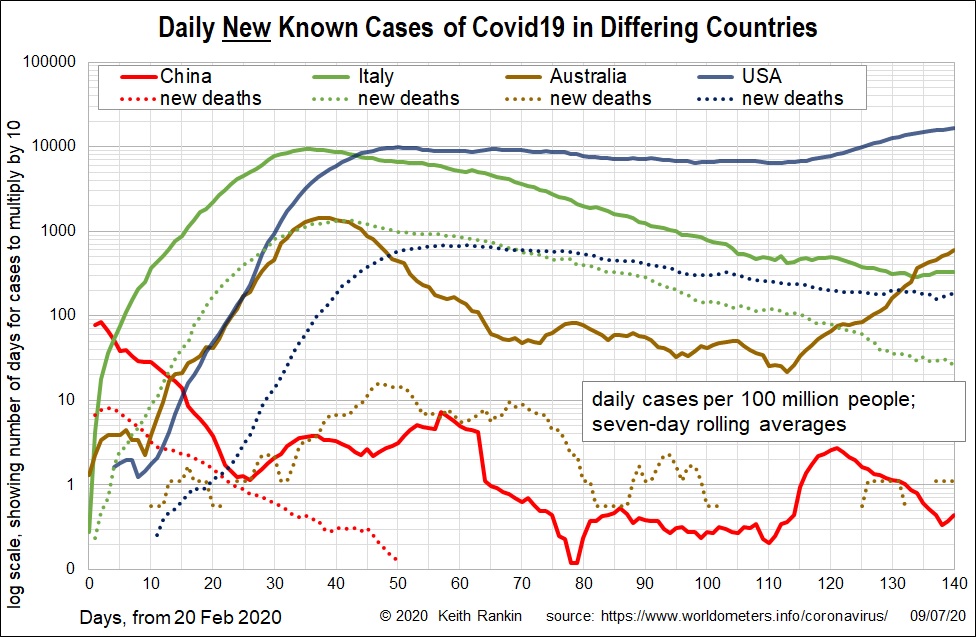
Chart 1 shows the first-wave in China, which in February was having nearly 100 daily cases per 100 million of the population, and upto 8 daily deaths per 100,000 people. It also shows the first-wave in Australia and USA (days 0 to 9), with a few resulting first-wave deaths (in early March; days 10 to 20).
Italy shows the classic single-wave covid curve, with a sharp exponential rise in cases for about 30 days, with deaths lagging by about 10 days. This is followed by a slow drawn-out downward exponential decline, with a bit of a plateau in new reported cases in the last few weeks (but with new deaths still declining).
Australia showed a similar but shorter exponential rise, ending with a peak an order of magnitude lower than Italy’s peak. Then Australia showed an exponential fall must faster than Italy’s. But Australia failed to eliminate Covid19, with new cases ticking over for many weeks, followed by the current Victoria outbreak. (In Victoria, the peak of the current outbreak is higher than its peak at the end of March.
The United States’ second-wave closely followed that of Italy; indeed, most of America’s early cases almost certainly came into New York from Milan in Italy. The decline in the United States was much slower than for the other countries; it took a couple of months for average daily cases to halve. Then, in early June, United States cases returned to a rising trend. Daily cases are now nearly double the May peak. However, American deaths have yet to show much of a rise. If Covid19 deaths turn up over the next week or so, then it will indicate a significant increase of the incidence of Covid19 in the USA. Otherwise, the rising case incidence may mainly reflect more testing, though it could be that new cases are mostly young adults.
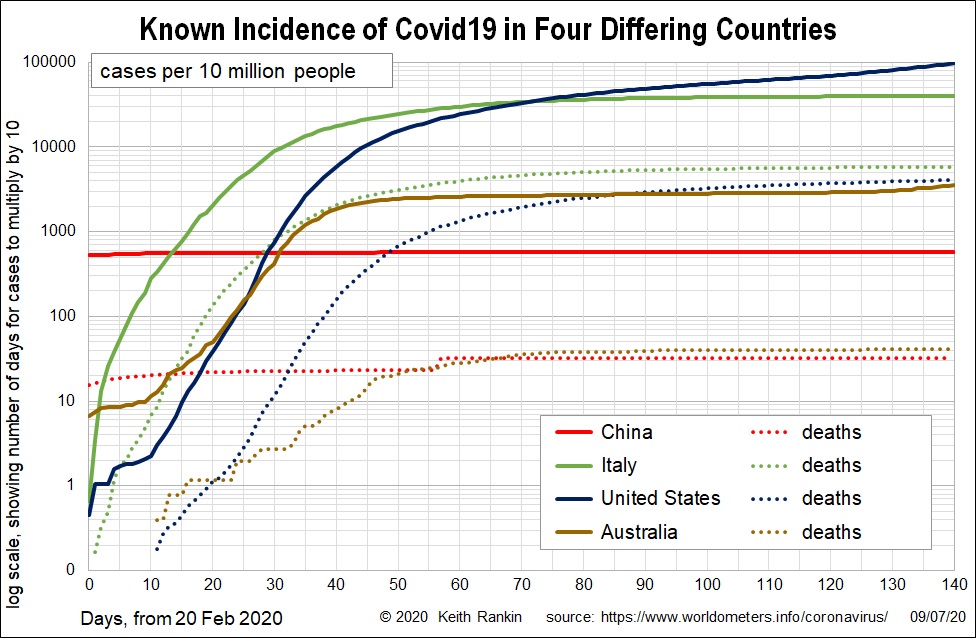
The second chart looks at accumulated cases, rather than new cases. It shows that Australian cases are six times higher than China’s. However, the death rates for the two countries are similar, meaning that China has a much bigger undercount than Australia. Indications are now revealing that – at least for economically developed countries with substantial elderly populations – the true case fatality rate is about one percent. That means deaths should be two orders of magnitude lower than cases. We see for Australia that the difference between deaths and cases is close to two orders of magnitude; so the reported data are close to the actual data. China’s true accumulated case incidence is probably a little more than half of Australia’s, perhaps 2,500 infections per 10 million people compared to Australia’s known 3,500 per 10 million. So China probably has four times more actual than known cases of infection.
In Chart 2, Australia is a close proximate for New Zealand, both for deaths and cases.
If we compare Italy and the United States, the undercount of infections looks higher for Italy. United States deaths are sitting at 3,000 per 10,000,000 people. If actual cases are 100 times higher (two orders of magnitude), they should be showing 300,000 on the chart (instead of the 100,000 shown). So, the actual case numbers in USA are about three times higher than the confirmed case numbers. If we multiply Italy’s deaths by 100, as we did for USA, then we get almost 500,000 infections in Italy per 10 million people; that’s five percent of the Italian population.
While Italy and USA have many infections (both between three and five percent infected), that indicates between 95 and 97 percent of people not infected; well short of ‘herd immunity’. To achieve herd immunity without an effective vaccine, deaths in Italy and the USA will need to increase by an order of magnitude (ie tenfold); maybe deaths would need to increase by more than that in the United States (and Mexico) where obesity is known to be a significant public health problem.


{kind=link}