
Source: The Conversation (Au and NZ) – By Rod Jackson, Professor of Epidemiology, University of Auckland

GettyImages
With vaccination rates still too low in Auckland and around Aotearoa New Zealand, and with unexpected cases still showing up, there are few options ahead of today’s government decision on alert levels.
Until there are high levels of immunity, any relaxation of restrictions within Aotearoa when Delta is in the community will dramatically increase the speed at which the virus spreads through the population.
The time has come for a concerted vaccination drive, mandatory vaccination for more workers, and a clear signal that eligible but unvaccinated people will face restricted access to travel and other activities.
With Delta, there is no “herd immunity” — almost everyone who has not been vaccinated will eventually (and sooner rather than later) get infected. Vaccinated people are about 75% less likely than unvaccinated people to develop a COVID infection if exposed, and over 90% less likely to develop severe disease.
In the current Auckland outbreak, only 3% of the more than 1,000 cases were fully vaccinated. There has been only one fully vaccinated patient among the more than 100 hospitalised cases.
With fewer than 10,000 New Zealanders having been infected by COVID-19, unlike most other countries we are completely dependent on high levels of vaccination to provide high levels of immunity.
System overload
Left to its own devices, Delta spreads like wildfire – from 1 person to 6, to 36, to 216, to 1296 and so on – at high speed until there is a high enough vaccination level. This rapid exponential spread is the main threat to health and other essential services.
No hospital system, however many ICU beds per capita, could cope, and no amount of testing would be able to get on top of Delta in an opened-up Aotearoa. Contact tracing systems would be overwhelmed in days.
Without a high vaccination level, increasing hospital capacity or investing in new drugs would be the equivalent of rearranging deck chairs on the Titanic.
Beyond the hospitals, COVID will spread through the unvaccinated 5–11-year-olds at school, who will then infect their teachers, parents and grandparents. Who will be able to care for whom?
Beyond the schools, businesses with clusters of unvaccinated staff will shut down because up to half the unvaccinated infected people will be too sick to work, and up to one in ten could be hospitalised. Asymptomatic infected staff will infect other staff, clients, customers and their families and friends.
Then there is long COVID. A large British study has reported one in three hospitalised COVID cases needed to be readmitted.
In another British study, more than half admitted to hospital had long COVID symptoms three months after discharge. Symptoms were worse among those aged under 50, women and those with higher pre-COVID fitness levels.
What are the acceptable costs?
Every national and international health authority has always accepted the only possible sustainable way to deal with COVID is through the development of immunity.
Since the introduction of safe and effective vaccines, every health authority has recommended high levels of vaccination as the only safe and acceptable way to achieve high levels of immunity.
Today, in semi-vaccinated Aotearoa, only two questions are relevant to any plan to open up:
- is there a high target vaccination level and what does the target imply about the numbers of infections, hospitalisations, deaths and cases of long COVID considered an “acceptable cost” of opening up?
- how does the plan propose to achieve the vaccination target required to meet the “acceptable cost”?
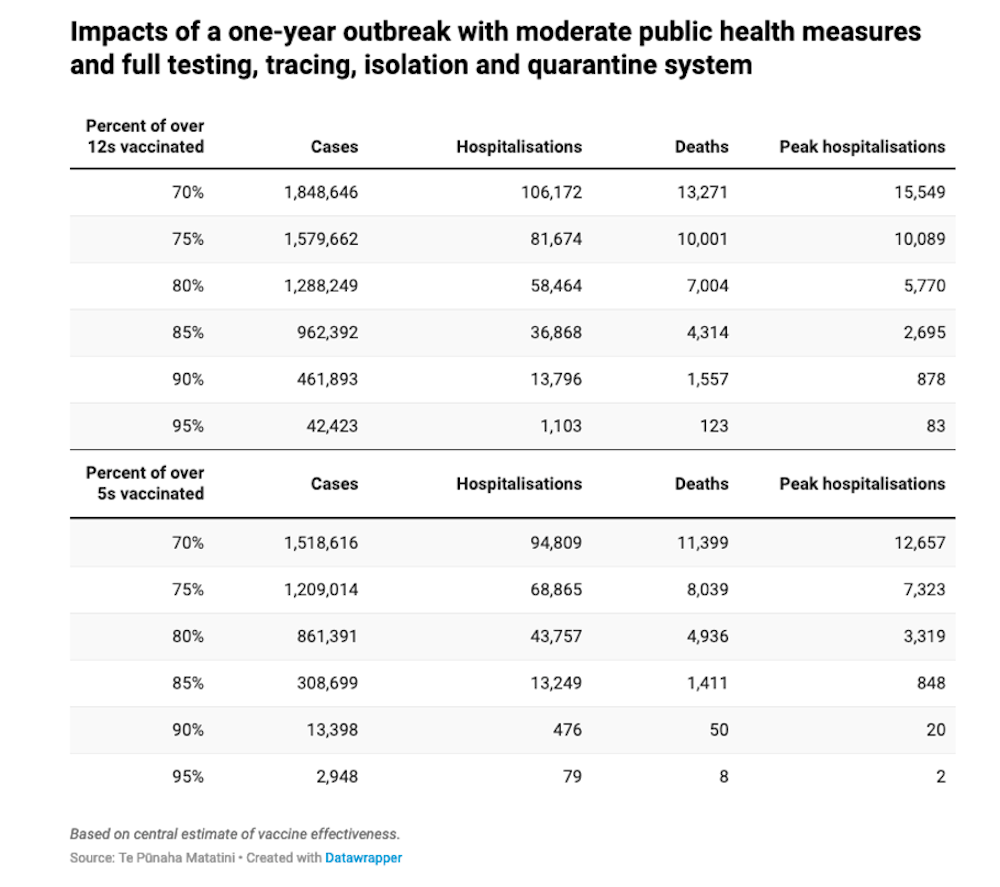
Aotearoa’s most respected COVID-19 modellers, from Te Pūnaha Matatini, have provided robust scenarios of the likely impacts of a one-year outbreak at different vaccination levels.
Their modelling assumes moderate public health measures, including a full testing, tracing, isolation and quarantine system. Their predictions are remarkably similar to equivalent predictions from Australian modelling groups (aside from the one used by the federal government).
More radical plan needed
The National Party’s recently announced “Opening Up” plan was based on nationwide lockdowns no longer being necessary when 70-75% of the population aged 12+ are fully vaccinated.
Based on the Te Pūnaha Matatini models, this suggests the acceptable cost, in the event of a new outbreak, would be somewhere between 1.5 million and 1.8 million cases, 80,000–105,000 hospitalisations and 10,000–13,000 deaths annually.
The plan states international borders would open at a 12+ vaccination level of 85-90%. It’s unclear why there are different thresholds for opening internally and externally. If COVID comes back, whether through an opened border or under the current border restrictions, the consequences will be the same without lockdowns.
National’s proposals for increasing vaccination rates are excellent, although most are already happening to a greater or lesser extent. If the government hasn’t already done so, however, the proposal to order a supply of booster shots should be adopted immediately, as we are very likely to need these as immunity wanes.
The key problem with the plan is that it’s not sufficiently radical to achieve either the 85-90% target or the more humane target of 95% or higher. Even at 95%, there could be 40,000 cases, 1,000 hospitalisations, over 100 deaths and over 10,000 cases of long COVID.
Vaccine ‘passports’ now
In most countries that have already achieved targets above 90%, the main motivation has been fear due to daily exposure to death and hospitalisations. Fortunately, this does not apply in New Zealand yet, although it might if lockdowns were removed as a strategy at 70–75% vaccination rates.
The most effective intervention now required to convince the last 20% of the eligible population to be vaccinated will be some form of vaccination authentication — a vaccine “passport”.
Internationally, this approach has been very successful. It has included mandatory vaccination in many jobs beyond border or healthcare, and restricted access to flying, hospitality and other activities for unvaccinated eligible people.
Both major parties have so far only hinted at many of these options, other than that vaccination should be mandated for healthcare workers. This should have been implemented months ago.
A non-partisan approach
It is not surprising politicians are reluctant to make vaccination compulsory for some, restrict activities for the unvaccinated, or allow businesses to exclude workers, clients and customers if they are unvaccinated. But we won’t achieve an acceptable target without it.
Among other international precedents, Victoria will require all school and childcare staff to have their first shot or a booking by October 18. In the US, all federal workers must be vaccinated by November 22. And vaccine “passports” are already required for access to hospitality in much of Western Europe.
New Zealand now needs a unified, non-partisan and radical approach to achieving a minimum 95% of eligible people vaccinated. Ideally this will include 5-11-year-olds if the Pfizer vaccine is approved for this age group.
Mandated vaccination for a wide range of jobs should be introduced, and limits on various activities put in place for unvaccinated eligible people. These may only be required for 12 months, but without them the current restrictions will have to remain.
With almost 80% of all eligible New Zealanders already having had their first vaccination shot, the country will be overwhelmingly behind such a proposal.
![]()
Rod Jackson does not work for, consult, own shares in or receive funding from any company or organisation that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.
– ref. NZ needs a more urgent vaccination plan — with nearly 80% now single-dosed, the majority will support it – https://theconversation.com/nz-needs-a-more-urgent-vaccination-plan-with-nearly-80-now-single-dosed-the-majority-will-support-it-168926


{kind=link}