Source: The Conversation (Au and NZ) – By Michael Baker, Professor of Public Health, University of Otago

Shutterstock/Photos Brian Scantlebury
February 28 marks three years since COVID was first reported in Aotearoa New Zealand. Since then there have been major advances in our understanding of this infection and the tools and strategies to combat it.
Here we describe three big opportunities to improve our response as we enter the fourth year of the pandemic.
Strategy is key to driving down infection
New Zealand’s response strategy started with elimination, which minimised infection and death from COVID during the first two years of the pandemic.
It also allowed time to roll out vaccines and improve treatments before widespread infection during the pandemic’s third year. These measures decreased the case fatality risk from about one in a hundred during the first two years to less than one in a thousand now.
The net effect was the lowest cumulative excess mortality in the OECD during this period.
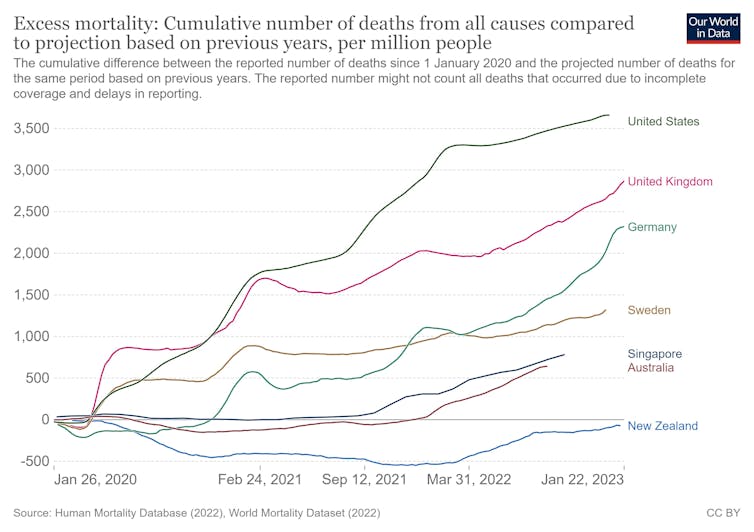
Our Word in Data, CC BY-SA
The world is now transitioning from an emergency pandemic response to treating COVID as another important infectious disease to be controlled. The first big challenge is identifying an optimal strategy for managing infection now that COVID is always present.
Elimination is not currently feasible with available and acceptable interventions, so the decision is about the optimal level of control from suppression to mitigation. This is a risk assessment question based on acute and long-term impacts of COVID infections.
In 2022, COVID became the second leading cause of death in New Zealand, behind ischaemic heart disease. Globally, it is likely to have been the third leading cause of death for the past three years (2020-22).
The immunity resulting from the cumulative effects of vaccination and prior exposure is reducing the severity of infection. Unfortunately, the evidence from multiple strands of research is that COVID infection is a multi-organ disease with symptoms commonly persisting after three months.
Infection may damage the circulatory system, brain and lungs. It also increases the risk of subsequent heart attacks and other circulatory diseases and appears to be driving an increase in excess mortality in many countries.
COVID is not influenza, where symptomatic infections typically occur years apart. With COVID, reinfections are common, and each carries a risk of illness, hospitalisation, death and disability from long COVID.
The life-course effects of experiencing multiple infections are not yet known.
This evidence supports a suppression strategy to minimise the frequency of infections and reinfections. Major international reviews describe this as a vaccines-plus approach which uses a mix of control measures as well as vaccines.
New Zealand has partially adopted this approach but will need to do more and clearly articulate a suppression strategy as a unifying goal for selecting interventions.
Effective and equitable delivery is critical
It can be argued we should treat COVID more like other infectious diseases. The converse strategy is that we should treat other infectious diseases more like COVID.
There is a convincing argument for an integrated approach to respiratory infections that builds on the co-benefits of addressing multiple infections, along with a strong emphasis on equity.
In the past we have accepted the annual death toll of around 500 from influenza and its big impact on our hospital system. Yet influenza largely disappeared during the time of COVID, in New Zealand and some other countries, even those with less stringent control measures. This finding shows that the burden of influenza is not inevitable.
We need to identify the most effective and cost-effective mix of respiratory protections. Examples include targeted and universal vaccine programmes, improved ventilation in public buildings and strategic mask use in enclosed public environments (for example, public transport).
These interventions need to be compared with other potential investments in health to decide the best use of available resources.
We know Māori and Pasifika have the highest rates of hospitalisation and death from COVID and lower levels of vaccination. This is a strong argument for continuing to strengthen Māori health leadership as exemplified by the new Māori Health Authority Te Aka Whai Ora.
An integrated programme addressing respiratory infections would be strengthened by research and surveillance. It is important to understand and address barriers to achieving high population coverage of key interventions. We also need ways to combat disinformation to help sustain the social license for public health measures.
High-quality integrated surveillance of respiratory infections would supply data on epidemiology, genomics and health equity.
We must learn and prevent the next pandemic
Given the extreme disruption the pandemic has caused, it is vital to learn from the experience. The terms of reference for the Royal Commission of Inquiry into New Zealand’s COVID response have a strong focus on managing future pandemics.
This goal is important as there are multiple infectious agents with pandemic potential. Avian influenza is a growing concern at present.
In our view, the greatest lesson from COVID is that elimination should be the default choice for future pandemics. A key priority is rapid elimination at source, followed by slowing the spread to give time to develop effective vaccines and other prevention measures.
As we enter the fourth year of the pandemic, there is cause for optimism.
Evidence supports a suppression strategy that minimises the frequency of infections and their harmful consequences. Delivering such a strategy is likely to be more effective, equitable and sustainable if combined with a broad programme which treats all serious respiratory infections more like COVID.
While the threat of future pandemics may be increasing, we now have the ability to eliminate them. This is a huge advance in global health security.
![]()
Michael Baker’s employer, the University of Otago, receives funding for his research on Covid-19 and other infectious diseases from the Health Research Council of New Zealand and the New Zealand Ministry of Health.
Amanda Kvalsvig’s employer, the University of Otago, receives funding for her research on Covid-19 and other infectious diseases from the Health Research Council of New Zealand and the New Zealand Ministry of Health.
Matire Harwood works for the University of Auckland. She receives funding from Health Research Council. She is affiliated with Papakura Marae Health Clinic, Accidental Compensation Corporation, Medical Research Institute of New Zealand and MAS Foundation.
– ref. It’s been 3 years since COVID entered New Zealand — here are 3 ways to improve our response – https://theconversation.com/its-been-3-years-since-covid-entered-new-zealand-here-are-3-ways-to-improve-our-response-196723