Source: The Conversation (Au and NZ) – By John Donne Potter, Professor, Research Centre for Hauora and Health, Massey University
Getty Images
Almost three years into the COVID pandemic, it clearly isn’t over.
New offshoots of the Omicron variant of SARS-CoV-2 continue to proliferate worldwide. The virus is mutating extensively and convergently (meaning the same mutations are popping up along different family trees) and, as a result, we now have what is increasingly being called a “variant soup”.
The current range of immunity-evading descendants of the Omicron variant is unprecedented in its diversity, which makes it harder to predict coming waves.
Although some may feel infection has now become inevitable, we must not forget that vaccination substantially lowers the risk of infection (including Omicron), hospitalisation and death, and staying free of infection means not having to face the risk of long COVID.
Vaccine protection is even better after receiving at least one booster, compared with just having the primary series. This is why Aotearoa New Zealand needs to embark on another round of boosters to better protect the population.
At present, just over 90% of the population aged 12 years or older have completed the primary course. More than 70% aged 18 or older have received the first booster, but only just over 40% of those over 50 have received the second booster. We look like an increasingly vulnerable population.
What we also need now, but do not yet have, is a sterilising vaccine of the sort we have for measles. This kind of vaccine eliminates the pathogen before it can replicate. The vaccinated person does not get ill, nor can they pass it on to others. Research is underway, including in New Zealand, but we are not there yet.
The variant soup and waning immunity
The growing prevalence of the variant soup in the US is clear from the latest data.
We don’t yet have a clear idea of the differences in transmissibility and severity among the new variants, although there are hints from France that the dominant new variant, BQ.1.1, and its sub-variants do not cause as much severe disease as we have seen earlier.
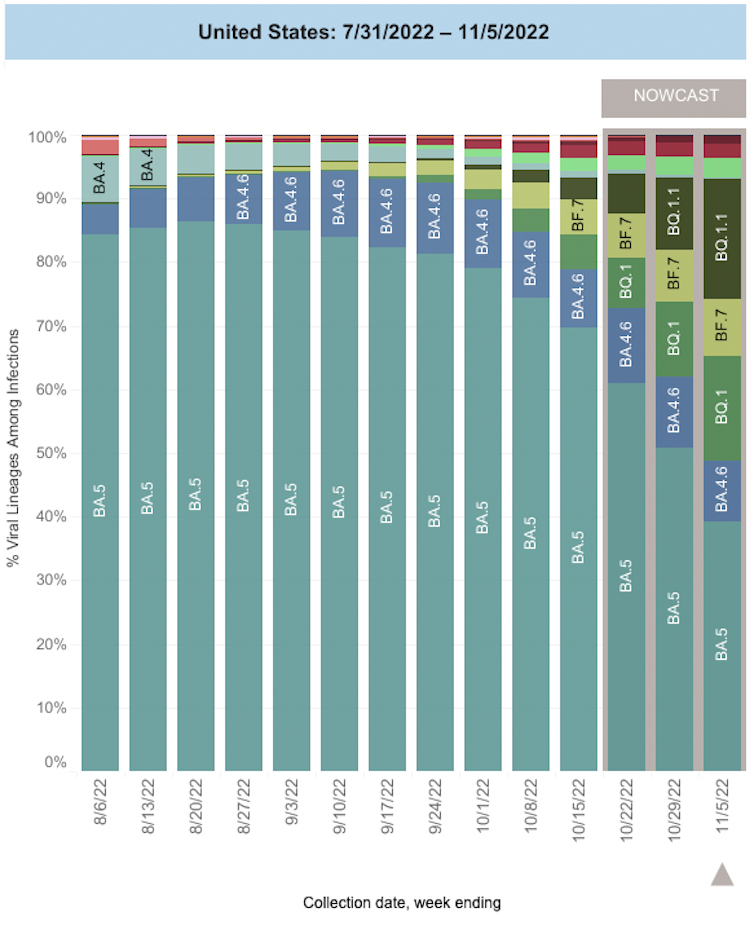
Author provided
We do know that immune responsiveness and vaccine effectiveness against Omicron sub-variants fade rapidly. The later variants have been better able to evade immunity than earlier ones.
The new variants have the same collection of mutations, which shows they are being selected for by the host (human) immune response, which in turn is influenced by our collective vaccination and infection history. The most immunity-evasive variants are BQ.1.1 (the most rapidly increasing variant in the US), XBB and BA.2.75.2.
As immunity wanes and as the virus mutates, we should take our guidance from how we handle these issues with other infectious diseases. Because tetanus immunity wanes, we get a booster every ten years. Because influenza viruses both mutate and re-emerge regularly as different variants, we get a yearly influenza vaccination as our best, albeit imperfect, protection against severe illness.
Read more:
Five reasons why young people should get a COVID booster vaccine
Do the new boosters work?
Small early studies, which are not yet peer reviewed, suggest the new bivalent boosters (targeting more than one Omicron variant) result in about the same level of neutralising antibodies as monovalent boosters.
However, one study, which used a more appropriate way of assaying (live virus rather than pseudo-virus), showed robustly higher neutralising antibody responses to recent variants, compared to monovalent boosters.
The fact that boosters raise protection overall, and that the bivalent version may do so even against recent variants, means making them available is crucial to us as individuals and as a community.
Boosters as the best strategy
The strongest immunity seems to arise as a result of vaccination and a breakthrough infection. This finding has resulted in a tendency towards advising that the best strategy is to be vaccinated and to become infected.
Such a hope-based strategy might obviate – after some ill-defined number of vaccinations and an ill-defined passage of time – the need for a further booster. Eventually, if we follow this line of reasoning, vaccination and other public-health measures might no longer be needed.
This is a strategy that fits our desperate need to no longer have to deal with this pandemic: many of us are in deep denial about the pandemic’s ongoing threat.
Even more, we are in denial about the pandemic eventually morphing into a new influenza-like endemic disease with recurring waves, probably with a higher risk of long COVID.
We’ll probably see a permanent new entity in our biological environment. But given our multi-generational experience of specific infectious diseases disappearing entirely or largely from our environment, definitely in the developed world and in some cases in the whole world, our denial means we are really not ready to “welcome” a new one in.
This denial is futile. The virus is neither sentient nor capable of responding to our wishes. Even if we were all willing to pursue the vaccination-plus-infection strategy, there is a price to pay for individuals and whānau – and for the healthcare system. That price is a growing burden of long COVID syndromes, which we don’t yet understand well – and certainly don’t manage well.
As the proportion of reinfections is going up (currently at 17% of daily cases) and the variant soup looms, we need to provide another round of boosters supported by clear reasons: to protect the most vulnerable; to reduce the risk of severe disease, hospitalisation, intensive care and death; to reduce the likelihood of long COVID; and to ensure our already stressed healthcare system is not overwhelmed.
We also need to strengthen our commitment to public-health measures: masks, distance and better ventilation. These have, to date, protected us quite well in Aotearoa and even better in countries like Japan that learned these lessons a century ago and have embedded them deeply in the social structure.
![]()
John Donne Potter does not work for, consult, own shares in or receive funding from any company or organisation that would benefit from this article, and has disclosed no relevant affiliations beyond their academic appointment.
– ref. With a COVID ‘variant soup’ looming, New Zealand urgently needs another round of vaccine boosters – https://theconversation.com/with-a-covid-variant-soup-looming-new-zealand-urgently-needs-another-round-of-vaccine-boosters-193616