
Data and Analysis by Keith Rankin.

The table below uses raw-death data published downloaded from https://ourworldindata.org/grapher/excess-mortality-raw-death-count to predict what death numbers would have occurred in 2020 and 2021 had there been no Covid19 pandemic. The actual death numbers are compared with the predicted (counterfactual) numbers to calculated excess deaths. These countries are sorted from the one with most deaths per person (Peru) to that with the fewest deaths per person to date (New Zealand).
This is of course an interim table; the deaths attributable to the pandemic – even in these countries – are far from over. ‘Deaths attributable’ are not the same as deaths clinically diagnosed as Covid19. The pandemic affects non-covid death rates as well. Typically, public health restrictions reduce immediate non-covid deaths, but may contribute to higher than otherwise expected future deaths. This varies from delayed diagnoses and treatments for conditions such as heart disease and cancer, to effects associated with changes in mental health, to health consequences arising from the economic impact of the pandemic. Countries can also expect to experience different incidences of other infectious diseases. There may also be losses – or gains – to people’s ‘quality of life’ that cannot be assessed simply through mortality statistics.
This data source excludes countries for which death statistics are unreliable or incomplete. Most of these countries are in Asia and Africa. In addition, I have excluded countries for which the data is not recent enough, or (mainly Asian countries) for which the major Covid19 outbreak is too recent to show up in the available data.
We should also note that only a small proportion of these deaths are due to the ‘delta strain’ of Covid19; indeed most deaths in most listed countries are due to the original ‘Wuhan strain’, which struck Europe with a vengeance in the autumn months of 2020 and continued into the New Year. Most European countries also experienced severe ‘alpha’ outbreaks. Most Latin American countries suffered substantially from the ‘gamma strain’ of Covid19.
By far the worst affected so far by Covid19 are countries in East Europe and Latin America. The worst affected outside of these two regions is Italy. Of the world’s really large countries, the worst are Russia, Mexico and Brazil.
In most countries, to date non-covid deaths have fallen. In a few countries, the reduction in non-covid deaths is bigger than the level of covid deaths, meaning that excess deaths are negative. These are mainly countries in Scandinavia and Oceania. Of these countries, Denmark may have essentially come through the pandemic, while New Zealand and Australia may only be at the beginning of their Covid19 experience. While New Zealand looks good so far in terms of excess deaths, a matter of concern is its higher overall death rates in 2019 and 2020 than Australia, a country with very similar age demographics and life expectancy.
The demographics of countries in different regions of the world can be very different. For example, the general pattern in Eastern Europe is for a falling and aging population; hence deaths as a percent of the population were already very high before Covid19, and have been even higher since. By contrast, countries in Latin America have growing and young populations. While western Europe falls in between, the ‘Anglosphere’ countries – United States, United Kingdom, Canada, Australia, Ireland, New Zealand – have younger populations than those in Europe.
The following table reflects Covid19’s excess death toll in terms of information available in September 2021.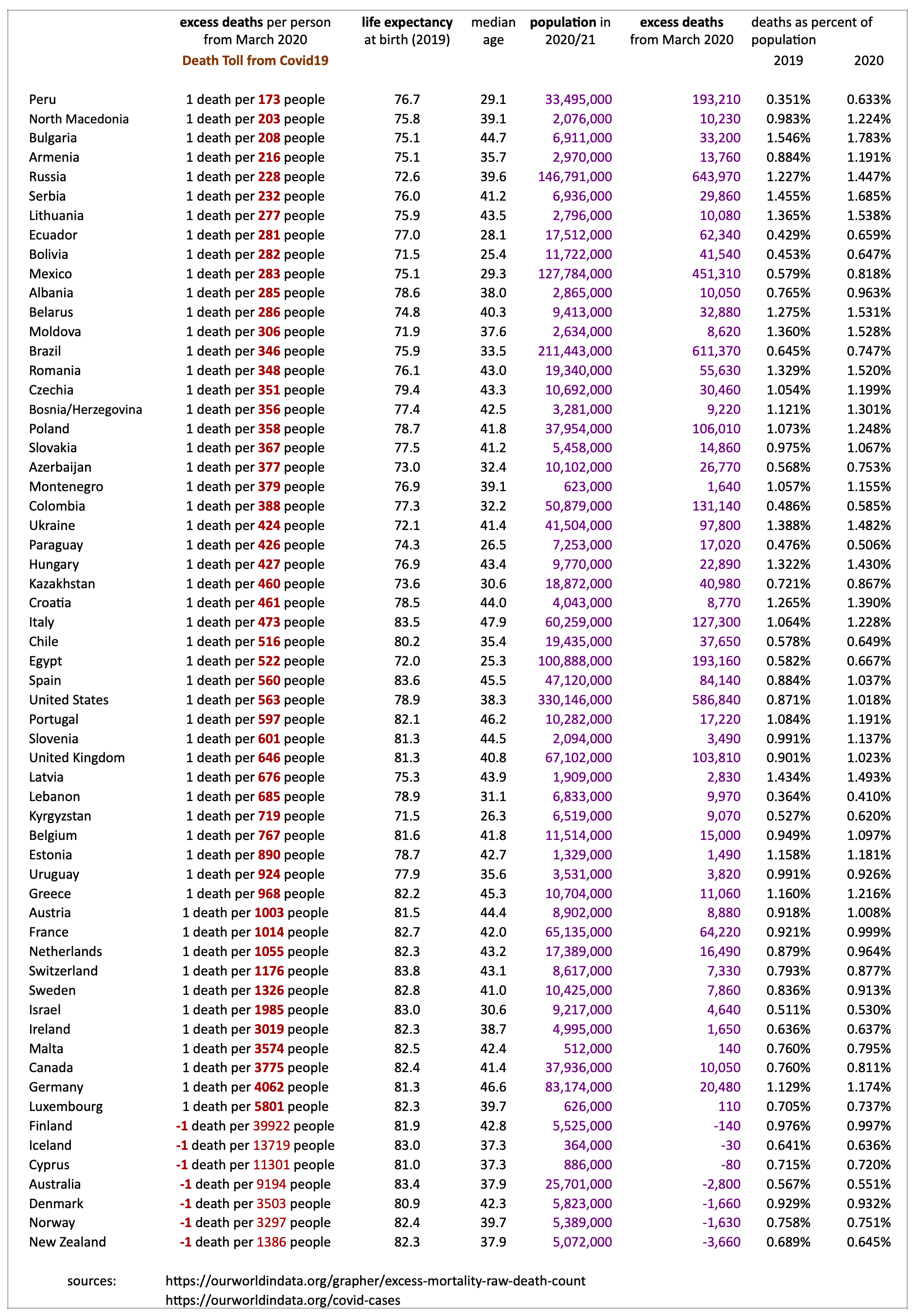
While the figures generally speak for themselves, it is important to note that the same pathogen has had very different impacts in different countries. And that those more prosperous countries which were first affected have by no means been the countries worst affected. We should also note that while all countries have taken some ‘barrier’ public health restrictions to defend themselves against the Covid19 pathogen – lockdowns, quarantines, physical distancing, facemasks – some countries that have implemented fewer such restrictions (such as Netherlands and Sweden) have achieved better outcomes than some much stricter countries. Denmark is coming to look like the exemplar country, which took strong protective measures in 2020, but also seems to have best-timed the removal of its emergency public health restrictions.
It is increasingly looking like the impact of Covid19 pandemic is going to be in proportion to the vulnerability of each country’s resident population, rather than to mutating strains of the pathogen; and noting that each country’s experience of the pandemic alters its vulnerability, commonly increasing its vulnerability to future pathogenic ‘attack’.
I will finish this note with a list of vulnerabilities:
- Low and/or falling immunity. While vaccinations significantly boost immunity, immunity – whether arising from infection or vaccination – itself diminishes over time; some immunities wane faster than others. Low or falling immunity to one pathogen of interest can, additionally, make a person vulnerable to other pathogens. Diminished exposure to endemic as well as epidemic pathogens reduces immunity to them. And diminishing general immunity increases vulnerability to inflammations and to non-infectious illnesses. People who already have such other health conditions are ‘comorbid’, are therefore less immune; they are more vulnerable to any pathogen in circulation. Clearly eastern countries in the European Union – such as Poland and Czechia, which largely missed Covid19’s first European wave – were more vulnerable to Covid19 in September 2020 than they were in March of that year; it seems likely that precautions they took earlier in 2020 aggravated the outcomes they faced later in 2020.
- Economic stress. This includes both poverty and inequality, and is manifest through various indicators of living conditions, such as housing, unemployment, underemployment, overemployment, inflation, malnutrition, food insecurity, access to healthcare, and immigration status. In and after a pandemic, levels of economic stress are not only high, but they are also changing. Historically much economic stress is relieved by migration to cities, to other provinces, or to other countries. We may note that one of the major reasons why most East European countries have populations that are old and poor is that most have experienced longstanding unresolved economic stresses which have induced substantial emigration. An important component of economic stress is excessive exposure – potentially lifelong exposure – to competitive market forces. While the marketplace plays a role in all of our lives, our lives should be much more than our struggles to achieve a living income. Economic stress also includes the marketing pressures we are placed under.
- Adversarial stress. This results from different people responding by coalescing into different ‘tribes’ which may act as information echo-chambers. The stress arises from people having to interact in some way with people affiliating with other tribes, or other factions of one’s own tribe. At its more extreme, adversarial stress includes invasions, civil wars, and political insurrections.
- Bureaucratic stress. This involves the many interactions with governments, and their associated rules and compliance procedures. It also involves regular interactions with non-government agents – especially employers and managers – who may themselves be undergoing substantial (and changing) bureaucratic stress. One major source of bureaucratic stress is the impediments placed by governments and adversaries onto people attempting to migrate their way to better lives. Another source of bureaucratic stress may be the enforced compliance with public health restrictions, all of which have costs as well as benefits, and some of which may have disputable benefits.
- Family stress. Having to deal with the stresses faced by or perpetrated by cohabitants (mainly family members). This can extend to having to provide support under sub-optimal conditions to high-needs people for which a caregiving person – and increasingly only that person – has a duty of care towards. While it may in reality require a village (or equivalent) to care for a needy person, in stressed societies the care of many needy people may be allocated, by default, to just one stressed person. Family stress will also arise where one or more people are afraid of another person or persons in their household.
- Mental unwellness. This can be a catch-all condition that both reflects the lonely desolation of material affluence, lack of personal autonomy, lack of sympathetic empathy, the absence of opportunities to live smaller less frenzied lives, and claustrophobic living conditions. And it reflects the accumulation of economic, adversarial, bureaucratic and family stresses. Too much stress can place an intolerable burden on the human nervous system.
It is these changing vulnerabilities that make people – and whole populations – at risk from a pandemic. The eventual Covid19 toll will reflect all these vulnerabilities.
————-
Keith Rankin (keith at rankin dot nz), trained as an economic historian, is a retired lecturer in Economics and Statistics. He lives in Auckland, New Zealand.