Source: The Conversation (Au and NZ) – By Michael Bennett, Professor in School of History and Classics, University of Tasmania
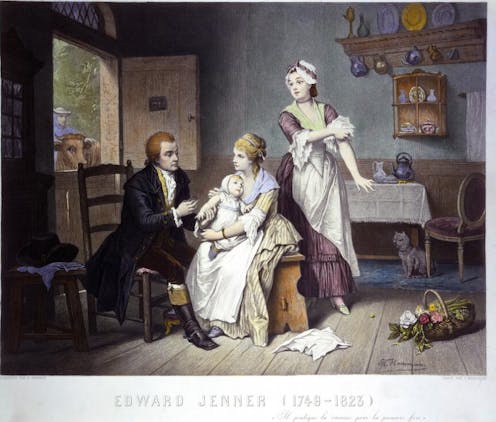
Edward Jenner vaccinating his son, held by Mrs Jenner; a maid rolls up her sleeve, a man stands outside holding a cow. Coloured engraving by C. Manigaud after E Hamman. The Wellcome Collection.
As the roll-out of COVID vaccines proceeds, it’s worth looking back on the challenges and successes of the early global spread of smallpox vaccination.
Smallpox (also known by its scientific name, variola) was a horrible, highly infectious disease, with a case fatality-rate of 30%. In 1798, Edward Jenner, an English country doctor, published data on cowpox (or “vaccine”, a term derived from the Latin for cow and increasingly preferred by Jenner; modern scientific name vaccinia). His data suggested this pustular disease found on dairy cows protected people from smallpox.
He detailed experiments in which he inoculated children with cowpox (usually by nicking the arm and inserting cowpox pus under the skin), and presented the inoculation of cowpox as a safe and effective way to prevent smallpox.
Jenner’s claims were initially met with scepticism. Even in Britain, vaccination was not taken up on any scale until 1800. By this time, though, cowpox samples were being dispatched overseas and attracting great interest as a way to protect people against smallpox. By 1805, at the height of the Napoleonic Wars, people were already being vaccinated all around the world. By 1815, several million people, half of them outside Europe, had been vaccinated.
Sadly, however, the global eradication of smallpox was not achieved until the late 1970s.
Read more:
Four of the most lethal infectious diseases of our time and how we’re overcoming them
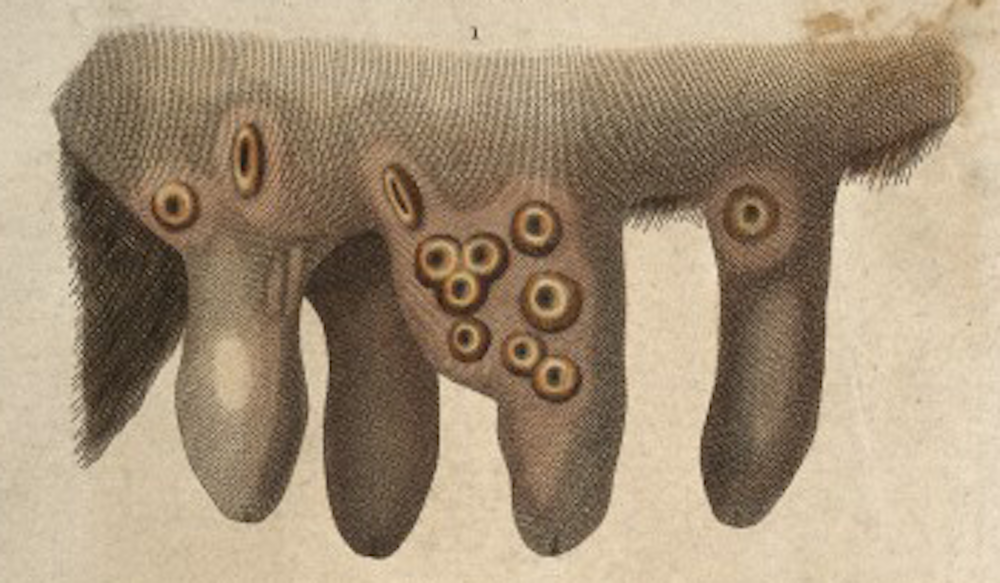
The wonder of cowpox
Smallpox was universally feared but people had learned to live with it. It was easy enough to recognise; victims became visibly ill before they became infectious. Crucially, people knew that if they survived the attack, they could be confident of lifelong immunity.
Learning to live with smallpox sometimes involved deliberately exposing children to the disease in the hope of a mild outcome. In Britain, it was found smallpox inoculation — that is, making a light cut in the arm and applying smallpox pus to the wound — resulted in far fewer deaths than in cases of naturally acquired smallpox.
It was as a practitioner of smallpox inoculation (which was also known as variolation) that Jenner found evidence people who had been casually infected with cowpox appeared to be immune to smallpox infection.
He put the theory to the test by inoculating a boy with cowpox lymph — taken not from the cow but from a vesicle or blister on a milkmaid’s hand — and demonstrating his resistance to smallpox by variolation.
Jenner’s presentation of cowpox as a safe and effective substitute for smallpox found corroboration in trials in London in 1799. It wasn’t easy to allay doubts among parents. Still, people were even more scared of smallpox, and recognised smallpox inoculation involved significant risk to the patient and the community. Cowpox was a game-changer.
More diaspora than roll-out
Although hailed as a boon, the new approach got off to a shaky start. Cowpox was rare, appearing only sporadically in dairy farms. The supply of vaccine depended from the outset on its propagation on human bodies. If the vaccine “took” on the child’s arm then, nine or ten days later, the ripe pustule was pricked to provide fresh vaccine.
Children of the poor were immunised at no charge and, on returning to clinics for examination, were put arm-to-arm with the next batch of children. Some vaccine was dried, often on cotton threads, as a future supply. Quality control was a major problem. In 1800, a cowpox institute was set up in London to propagate and distribute vaccine and in 1803 the Royal Jenner Society was established to promote the practice.
J. Pass, Public domain, via Wikimedia Commons
The spread of the first vaccine was more diaspora than roll-out. Samples of cowpox on cotton threads were sent in the post, in Britain and overseas, rather in the manner of plant seeds.
Many samples proved useless on arrival, but by sending them in some profusion, it proved relatively simple to seed the practice in Europe and North America. Improvements in packaging even made it possible to send vaccine from Vienna to Baghdad, where it was propagated for onward transmission to India in 1802. Viable vaccine was even delivered, after a 154-day voyage, to Sydney in 1804.
The world arm-to-arm
Another approach to conquering the tyranny of distance was to move patients under vaccination. Early in 1802, Tsar Alexander approved an expedition to establish vaccination through Russia in which children vaccinated in one province were escorted to go “arm-to-arm” with children in the next. In 1803, King Carlos of Spain launched an even grander expedition that, by vaccinating a succession of children, delivered live vaccine to Spanish America and then across the Pacific to Manila and Macao.
Vaccination literally brought the world arm-to-arm. The rapid global spread of the vaccine itself owed a lot to the universal dread of smallpox but also to humanitarian enthusiasm and international collaboration.
A range of measures were used to embed the practice. In Berlin, children were given trinkets and medals. Poor mothers in Mexico and India were bribed to have their children vaccinated. In Austria, mothers whose children died of smallpox were named and shamed.
Some states moved rapidly along the road to compulsion. In France, where Napoleon was a great advocate of the practice, vaccination was urged as a civic duty but not made mandatory. In Denmark, a vaccination certificate was rapidly made a requisite for schooling, public employment and even marriage.
Complacency and lack of resolve
Aware of vaccine’s global success, Jenner and his colleagues deplored the loss of momentum in Britain itself. In London, the practice was under challenge from a noisy anti-vaccination lobby led by old-style inoculators.
A smallpox epidemic in 1805, while showing the value of vaccination, disclosed some failures arising from poor early practice. In claiming vaccination was for life, Jenner had set the bar too high. To the end of his life in 1823, he was reluctant to concede the need for periodic re-vaccination.
The major problem in Britain and elsewhere was complacency. The early success in suppressing smallpox, and indeed eliminating it in some places, led parents to neglect vaccination.
Outbreaks in the 1830s were a major shock and pushed the British government to fund vaccination in 1840 and to make it mandatory in 1853. Victoria — though not New South Wales — followed this lead. Although it was controversial and fuelled anti-vaccination sentiment, compulsory vaccination, with some provision for conscientious objection, played a vital role making the practice routine. This kept smallpox at bay, prompted improvements, and helped inspire the development of new vaccines.
From the outset, vaccination was seen as a means of eradicating smallpox. It saved countless lives, kept communities safe for as long as vaccination was maintained, and limited the severity of outbreaks.
The permanent elimination of smallpox required governments to provide the infrastructure and resources, and show the political will to incentivise if not mandate vaccination.
Although the disease was largely brought under control in the West, millions were still dying from smallpox elsewhere in the middle of the twentieth century when the World Health Organization committed itself to the global eradication of smallpox.
Read more:
Four of the most lethal infectious diseases of our time and how we’re overcoming them
![]()
Michael Bennett has received support for his work on this topic from the Australian Research Council.
He is the author of War Against Smallpox. Edward Jenner and the Global Spread of Vaccination (Cambridge University Press, 2020).
– ref. Eradicating smallpox: the global vaccination push that brought the world ‘arm-to-arm’ – https://theconversation.com/eradicating-smallpox-the-global-vaccination-push-that-brought-the-world-arm-to-arm-162091

